1. Public health as a science and subject of teaching
1.1 Basic concepts and social conditioning public health
Public health and healthcare as an independent medical science studies the impact of social conditions and environmental factors on the health of the population in order to develop preventive measures to improve its health and improve medical care. Public health studies a wide range of medical, sociological, economic, managerial, and philosophical problems in specific historical conditions.
Unlike various clinical disciplines, public health studies the health status not of individuals, but of human groups, social groups and society as a whole in connection with conditions and lifestyle. At the same time, living conditions and industrial relations, as a rule, are decisive for people’s health. For example, socio-economic transformations, scientific and technological progress can bring certain benefits to society, but at the same time they can also have a negative impact on its health.
Discoveries in the field of physics, chemistry, biology, urbanization, rapid development of industry in many countries, large volumes of construction, chemicalization Agriculture etc. often lead to serious environmental violations, which have a detrimental effect, first of all, on human health. Therefore, one of the tasks of public health is to develop recommendations for the prevention of negative phenomena that negatively affect the health of society.
For the systematic development of the economy of any country, information about the size, age and sex structure of the population, and the determination of its forecasts for the future are of great importance. Public health identifies patterns of population development, studies demographic processes, forecasts the future, and develops recommendations for state regulation of population size.
Of key importance in the study of this discipline is the question of the effectiveness of the impact on the health of the population of all activities carried out by the state, and the role of healthcare and individual medical institutions in this.
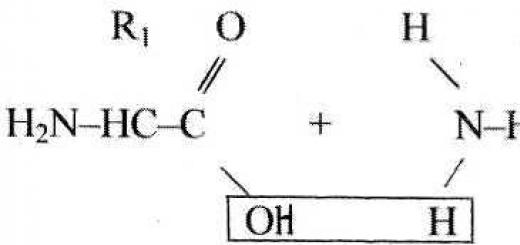
According to accepted concepts, medicine is a system of scientific knowledge and practical activities, the goals of which are to strengthen and preserve health, prolong the life of people, prevent and treat human diseases. Thus, medicine is based on two basic concepts - “health” and “disease”. These two concepts, while fundamental, are also the most difficult to define.
IN modern literature exists a large number of definitions and approaches to the concept of “health”.
The starting point for the medical and social interpretation of health is the definition adopted by the World Health Organization (WHO): “Health is a state of complete physical, spiritual and social well-being and not merely the absence of disease or infirmity.”
This definition is reflected in the WHO Constitution (1948). WHO has proclaimed the principle according to which “...the enjoyment of the highest attainable standard of health is a fundamental right of every person.”
In medical and social research, when assessing health, it is advisable to distinguish four levels:
first level – individual health – individual health;
second level – health of social and ethnic groups – group health;
third level – health of the population of administrative territories – regional health;
fourth level – health of the population, society as a whole – public health.
The characteristics of group, regional, public health in statics and dynamics are considered as an integral state of health of all individuals taken together. It should be understood that this is not just a sum of data, but a sum of interrelated quantitative and qualitative indicators.
According to WHO experts, in medical statistics, health at the individual level is understood as the absence of identified disorders and diseases, and at the population level - the process of reducing mortality, morbidity and disability, as well as increasing the perceived level of health.
Public health, according to WHO, should be considered as a resource of national security, a means that allows people to live prosperous, productive and high-quality lives. All people should have access to the resources they need to stay healthy.
Human health can be considered in various aspects: socio-biological, socio-political, economic, moral-aesthetic, psychophysical, etc. Therefore, now in practice terms have begun to be widely used that reflect only one facet of population health - “mental health”, “reproductive health”, “general somatic health”, “ecological health”, etc. Or – the health of a particular demographic or social group – “pregnant health”, “children’s health”, etc.
Although the use of these terms narrows the understanding of the classical definition of “public health,” they can be used in practice.
To assess individual health, a number of very conditional indicators are used: health resources, health potential and health balance.
Health Resources – These are the morphofunctional and psychological capabilities of the body to change the balance of health in a positive direction. Increasing health resources is ensured by all measures of a healthy lifestyle (nutrition, physical activity, etc.).
Health potential – this is the totality of an individual’s abilities to adequately respond to the influence of external factors. The adequacy of reactions is determined by the state of the compensatory-adaptive systems (nervous, endocrine, etc.) and the mechanism of mental self-regulation (psychological defense, etc.).
Health balance – a pronounced state of balance between health potential and the factors acting on it.
Currently, there are very few indicators that would objectively reflect the quantity, quality and composition of public health. All over the world, the search and development of integral indicators and indices for assessing the health of the population is underway. This is due to a number of reasons.
Firstly, correctly collected and well-analyzed statistical data on health serve as the basis for state and regional planning of health-improving activities, the development of organizational forms and methods of work of health authorities and institutions, as well as for monitoring the effectiveness of their activities in preserving and strengthening the health of the population.
Secondly, high demands are placed on integral indicators and indices of population health. WHO believes that these indicators should have the following qualities:
1. Availability of data. It must be possible to obtain the required data without carrying out complex special studies.
2. Comprehensiveness of coverage: The indicator must be derived from data covering the entire population for which it is intended.
3. Quality. National (or territorial) data should not vary over time and space in such a way that the indicator is significantly affected.
4. Versatility. If possible, the indicator should reflect a group of factors that are identified and influence the level of health.
5. Computability. The indicator should be calculated in the simplest possible way, and the calculation should not be expensive.
6. Acceptability (interpretability): The indicator must be acceptable, and there must be acceptable methods for calculating the indicator and its interpretation.
7. Reproducibility. When using a health indicator by different specialists in different conditions and at different times the results should be identical.
8. Specificity. An indicator should reflect changes only in those phenomena that it serves as an expression.
9. Sensitivity. The health indicator must be sensitive to changes in relevant phenomena.
10. Validity. An indicator must be a true expression of the factors of which it is a measure. Some form of independent and external evidence of this fact must be created.
11. Representativeness. The indicator must be representative in reflecting changes in the health of individual age-sex and other populations identified for management purposes.
12. Hierarchy. The indicator must be constructed according to a single principle for different hierarchical levels allocated in the population being studied for the diseases taken into account, their stages and consequences. There must be the possibility of its unified collapse and expansion according to its constituent components.
13. Goal consistency. The health indicator must adequately reflect the goals of maintaining and developing (improving) health and stimulate society to find the most effective ways to achieve these goals.
In medical and social research, to quantify group, regional and public health in our country, it is traditional to use the following indicators:
1. Demographic indicators.
2. Morbidity.
3. Disability.
4. Physical development.
Currently, many researchers are attempting to provide a comprehensive assessment of public health (quantitative and qualitative) and even develop special indicators for its assessment.
For example, American scientists, studying the health status of American Indians, developed an index that is a linear function of mortality and includes the number of days spent on outpatient and inpatient treatment. The index was then modified to assess the impact of disease on different population groups.
There is another approach that has been widely developed among American researchers - the model health status index. The modern approach to the integral assessment of population health is often associated with this model. The goals of creating this model were both to develop generalized indices of morbidity and mortality of the population, and to develop quantitative methods for measuring the effectiveness of various programs in the field of public health.
The basis of the concept of the health status index model is the representation of an individual’s health as a continuously changing set of so-called instantaneous health in the form of a certain value that takes values from optimal well-being to maximum illness (death). This interval is divided into an ordered set of health states - movement along the interval; population health – distribution of points characterizing people’s health over this interval.
One of the most popular is the index proposed by World Development Bank experts in a 1993 report to assess the effectiveness of investments in health care. In Russian translation it sounds like "global burden of disease (GBD)" and quantifies population losses in active life due to disease. The unit used to measure GBD is the disability-adjusted life year (DALY). The GBD measure takes into account the loss due to premature death, which is defined as the difference between actual age at death, life expectancy at that age and years lost healthy life as a result of disability.
The GBD calculation makes it possible to assess the significance of various diseases, justify healthcare priorities and compare the effectiveness of medical interventions in terms of the level of expenditure per year of life without disease.
However, the lack of necessary statistics to fill the models with actual data does not allow regular calculations of indices. Problems in determining the quantity and quality of public health are partly related to the fact that in medicine one cannot talk about health and illness in general, but one should talk about the health and illness of people. And this obliges us to approach a person not only as a biological, animal organism, but as a biosocial being.
Health modern man is the result of the natural evolution of the species Homo sapiens, in which social factors have a gradually increasing influence. Their role over the 10,000 years of civilization has increased in all respects. Man receives health, in a certain sense, as a gift of nature, he inherited it from his animal ancestors natural basis, a program of behavior in this world. However, in the process of socialization, the level of health changes either in one direction or the other, the laws of nature manifest themselves in a special form, characteristic only of man.
The biological never manifests itself in a person in a purely natural form - it is always mediated by the social. The problem of the relationship between the social and the biological in a person is the key to understanding the nature and nature of his health, his diseases, which should be interpreted as biosocial categories.
Human health and illness, in comparison with animals, is a new, socially mediated quality.
WHO documents have repeatedly indicated that human health is a social quality, and therefore, to assess public health, WHO recommends the following indicators:
1. Deduction of gross national product for health care.
2. Availability of primary health care.
3. Coverage of the population with medical care.
4. Level of immunization of the population.
5. The extent to which pregnant women are examined by qualified personnel.
6. Nutritional status of children.
7. Infant mortality rate.
8. Average life expectancy.
9. Hygienic literacy of the population.
Public health is determined by the complex influence of social, behavioral and biological factors. If we're talking about about the social conditioning of health, it is implied that social risk factors have a paramount importance, and sometimes a decisive influence on it.
The social conditioning of health is confirmed by numerous medical and social studies. For example, it has been proven that premature birth occurs 4 times more often in unmarried women than in married women; The incidence of pneumonia in children in single-parent families is 4 times higher than in complete families. The incidence of lung cancer is affected by smoking, environment, place of residence, etc.
Unlike the direct causes of diseases (viruses, bacteria, etc.), risk factors act indirectly, disrupt the stability of regulatory mechanisms, and create an unfavorable background for the occurrence and development of diseases. Thus, for the development of a pathological process, in addition to a risk factor, the action of a specific causative factor is also required.
Under the influence of a complex of factors, the value of public health indicators changes and sometimes quite significantly, both in space and time; they differ in individual age, gender, and social groups of the population, have regional characteristics and their own patterns of distribution, i.e. have their own epidemiology.
In modern literature, under the concept "epidemiology" most often understand the science that studies the patterns of occurrence and spread of pathological processes in order to develop measures for the prevention and optimal treatment of diseases. Epidemiology studies the influence of a complex of various factors on the formation of health, the prevalence of various diseases (infectious and non-infectious) and physiological conditions of a person.
Summarizing the above considerations, we can formulate the concept "epidemiology of public health", or "social epidemiology": is a section of the discipline “public health and healthcare” that studies the patterns of distribution of public health indicators in time, space, among various population groups in connection with the influence of conditions and lifestyle, and environmental factors.
The goal of public health epidemiology (social epidemiology) is the development of political, economic, medical, social and organizational measures aimed at improving public health indicators. In the future, when using this term, we will give it exactly this meaning.
1.2 History of the development of public health
Social-hygienic elements and prescriptions are found in the medicine of ancient socio-economic formations, but the isolation of social hygiene as a science is closely related to the development of industrial production.
The period from the Renaissance to 1850 marked the first stage in the modern development of public health (then this science was called “social hygiene”). During this period, serious research was accumulated on the interdependence of the health of the working population, their living and working conditions.
The first systematic manual on social hygiene was Frank's multi-volume work “System einer vollstandingen medizinischen Polizei”, written between 1779 and 1819.
The utopian socialist doctors who held leadership positions during the revolutions of 1848 and 1871 in France tried to scientifically justify public health measures, considering social medicine the key to improving society.
The bourgeois revolution of 1848 was important for the development of social medicine in Germany. One of the social hygienists of that time was Rudolf Virchow. He emphasized the close connection between medicine and politics. His work “Mitteilungen uber Oberschlesien herrschende Typhus-Epidemie” is considered one of the classics in German social hygiene. Virchow was known as a democratically minded doctor and researcher.
It is believed that the term “social medicine” was first proposed by the French physician Jules Guerin. Guerin believed that social medicine included “medical police, environmental hygiene and forensic medicine.”
Virchow's contemporary Neumann introduced the concept of “social medicine” into German literature. In his work “Die offentliche Gesundshitspflege und das Eigentum”, published in 1847, he convincingly proved the role of social factors in the development of public health.
At the end of the 19th century, the development of the main direction of public health to the present day was determined. This direction connects the development of public health with the general progress of scientific hygiene or, with biological and physical hygiene. The founder of this trend in Germany was M. von Pettenkofer. He included a section on “Social Hygiene” in the hygiene manual he published, considering it the subject of that area of \u200b\u200blife where the doctor meets with large groups of people. This direction gradually acquired a reformist character, as it was unable to offer radical sociotherapeutic measures.
The founder of social hygiene as a science in Germany was A. Grotjan. In 1904, Grotjan wrote: “Hygiene must... study in detail the influence of social relations, and social environment, in which people are born, live, work, enjoy, continue their lineage and die. So it becomes social hygiene, which acts next to physical and biological hygiene as its complement.”
According to Grotjan, the subject of social-hygienic science is the analysis of the conditions under which the relationship between man and the environment occurs.
As a result of such studies, Grotjan came closer to the second side of the subject of public health, that is, to the development of norms that regulate the relationship between a person and the social environment so that they strengthen his health and benefit him.
England also had major public health figures in the 19th century. E. Chadwick saw the main reason for the poor health of the people in their poverty. His work “The sanitary conditions of laboring populations,” published in 1842, revealed the difficult living conditions of workers in England. J. Simon, being the chief physician of the English health service, conducted a series of studies of the main causes of mortality in the population. However, the first department of social medicine was created in England only in 1943 by J. Raylem at Oxford.
The development of social hygiene in Russia was most contributed by F.F. Erisman, P.I. Kurkin, Z.G. Frenkel, N.A. Semashko and Z.P. Soloviev.
Of the major Russian social hygienists, it is necessary to note G.A. Batkis, who was a famous researcher and author of a number of theoretical works on social hygiene, who developed original statistical methods for studying the sanitary condition of the population and a number of methods for operating medical institutions (a new system of active patronage for newborns, the method of anamnestic demographic studies, etc.).
1.3 Subject of public health
The nature of the health care system in each country is determined by the position and development of public health as a scientific discipline. The specific content of any public health course varies depending on national conditions and needs, as well as the differentiation achieved by the various medical sciences.
The classic definition of the content of public health, mentioned in a discussion organized by WHO on the topic “Health Organization as a Scientific Discipline”: “... public health is based on a “tripod” of social diagnosis, which is studied mainly by the methods of epidemiology, social pathology and social therapy , based on cooperation between society and health workers, as well as on administrative and health-preventive measures, laws, regulations, etc. at central and local government bodies."
From the point of view of the general classification of sciences, public health is on the border between natural science and social sciences, that is, it uses the methods and achievements of both groups. From the point of view of the classification of medical sciences (about the nature, restoration and promotion of human health, human groups and society), public health seeks to fill the gap between the two main groups of clinical (therapeutic) and preventive (hygienic) sciences, which has developed as a result of the development of medicine. It plays a synthesizing role, developing unifying principles of thinking and research in both areas of medical science and practice.
Public health provides a general picture of the state and dynamics of health and reproduction of the population and the factors determining them, and from this the necessary measures follow. No clinical or hygienic discipline can provide such a general picture. Public health as a science must organically combine a specific analysis of practical health problems with research into the patterns of social development, with problems of the national economy and culture. Therefore, only within the framework of public health can a scientific organization and scientific planning of health care be created.
The state of a person’s health is determined by the function of his physiological systems and organs, taking into account gender, age and psychological factors, and also depends on the influence of the external environment, including the social one, with the latter being of leading importance. Thus, human health depends on the influence of a complex set of social and biological factors.
The problem of the relationship between the social and the biological in human life is a fundamental methodological problem of modern medicine. This or that interpretation of natural phenomena and the essence of human health and illness, etiology, pathogenesis and other concepts in medicine depends on its solution. The socio-biological problem involves the identification of three groups of patterns and the corresponding aspects of medical knowledge:
1) social patterns from the point of view of their impact on health, namely, on the morbidity of people, on changes in demographic processes, on changes in the type of pathology in various social conditions;
2) general patterns for all living beings, including humans, manifested at the molecular biological, subcellular and cellular levels;
3) specific biological and mental (psychophysiological) patterns inherent only to humans (higher nervous activity, etc.).
The last two patterns appear and change only through social conditions. Social patterns for a person as a member of society are leading in his development as a biological individual and contribute to his progress.
The methodological basis of public health as a science is the study and correct interpretation of the causes, connections and interdependence between the state of health of the population and public relations, i.e. in the correct solution of the problem of the relationship between the social and the biological in society.
Social and hygienic factors influencing public health include working and living conditions of the population, housing conditions; level of wages, culture and education of the population, nutrition, family relationships, quality and availability of medical care.
At the same time, public health is also influenced by climatic-geographical and hydrometeorological factors of the external environment.
A significant part of these conditions can be changed by society itself, depending on its socio-political and economic structure, and their impact on the health of the population can be both negative and positive.
Consequently, from a social and hygienic point of view, the health of the population can be characterized by the following basic data:
1) the state and dynamics of demographic processes: fertility, mortality, natural population growth and other indicators of natural movement;
2) the level and nature of morbidity among the population, as well as disability;
3) physical development of the population.
The study and comparison of these data in various socio-economic conditions allows us not only to judge the level of public health of the population, but also to analyze the social conditions and reasons that influence it.
In essence, all practical and theoretical activities in the field of medicine should have a social and hygienic orientation, since any medical science contains certain social and hygienic aspects. It is public health that provides the social and hygienic component of medical science and education, just as physiology substantiates their physiological direction, which is implemented in practice by many medical disciplines.
1.4 Public health methods
Public health like others scientific disciplines, has its own research methods.
1) Statistical method As a fundamental method of social science, it is widely used in the field of public health. It allows you to establish and objectively evaluate changes in the health status of the population and determine the effectiveness of the activities of health authorities and institutions. In addition, it is widely used in medical research (hygienic, physiological, biochemical, clinical, etc.).
Expert assessment method serves as a complement to the statistical one, the main task of which is to determine indirectly certain correction factors.
Public health uses quantitative measurements using statistics and epidemiological methods. This makes it possible to make forecasts based on pre-formulated patterns, for example, it is quite possible to predict future fertility, population size, mortality, mortality from cancer, etc.
2). Historical method is based on the study and analysis of public health and healthcare processes at various stages of human history. The historical method is a descriptive, descriptive method.
3). Economic research method makes it possible to establish the influence of the economy on healthcare and, conversely, healthcare on the economy of society. Health economics is an integral part of a country's economy. Health care in any country has a certain material and technical base, which includes hospitals, clinics, dispensaries, institutes, clinics, etc. Sources of health care financing and issues of the most effective use of these funds are researched and analyzed.
To study the influence of socio-economic factors on people's health, methods used in economic sciences are used. These methods find direct application in the study and development of such health issues as accounting, planning, financing, health care management, rational use of material resources, scientific organization labor in health authorities and institutions.
4). Experimental method is a method of searching for new, most rational forms and methods of work, creating models of medical care, introducing best practices, testing projects, hypotheses, creating experimental bases, medical centers, etc.
Experiments can be carried out not only in natural sciences, but also in social sciences. In public health, the experiment may not be used often due to the administrative and legislative difficulties associated with it.
In the field of healthcare organization, a modeling method is being developed, which consists of creating organizational models for experimental testing. Due to experimental method Greater reliance is placed on experimental zones and health centers, as well as experimental programs on individual problems. Experimental sites and centers can be called “field laboratories” for conducting health research. Depending on the goals and problems for which they were created, these models vary significantly in scope and organization, and can be temporary or permanent.
5. Observation and survey method. To replenish and deepen this data, special studies can be undertaken. For example, to obtain more in-depth data on the morbidity of people in certain professions, the results obtained during medical examinations of this contingent are used. To identify the nature and degree of influence of social and hygienic conditions on morbidity, mortality and physical development, survey methods (interviews, questionnaires) of individuals, families or groups of people can be used according to a special program.
Using the survey method (interview), you can obtain valuable information on a variety of issues: economic, social, demographic, etc.
6. Epidemiological method. Epidemiological analysis occupies an important place among epidemiological research methods. Epidemiological analysis is a set of methods for studying the characteristics of the epidemic process in order to determine the reasons contributing to the spread of this phenomenon in a given territory, and to develop practical recommendations for its optimization. From the point of view of public health methodology, epidemiology is applied medical statistics, which in this case acts as the main, largely specific, method.
The use of epidemiological methods in different areas of health care on large populations allows us to distinguish various components of epidemiology: clinical epidemiology, environmental epidemiology, epidemiology of non-communicable diseases, epidemiology of infectious diseases, etc.
Clinical epidemiology is the basis of evidence-based medicine, which allows, using strictly scientific methods based on studying the clinical course of the disease in similar cases, make a prognosis for each specific patient. The goal of clinical epidemiology is the development and application of clinical observation methods that make it possible to make objective conclusions, avoiding the influence of previously made errors.
Noncommunicable disease epidemiology studies the causes and incidence of noncommunicable diseases with the goal of developing preventive measures and reducing the prevalence of these diseases.
Epidemiology of infectious diseases studies the patterns of the epidemic process, the causes of the emergence and spread of infectious diseases in order to develop measures to combat these diseases, their prevention and elimination.
When talking about public health, we highlight the epidemiology of public health indicators.
To study various problems in the field of public health, it is necessary to use all of the specified research methods. They can be used not only independently, but also in a variety of combinations, thanks to which consistency and evidence of the results of social and hygienic research can be achieved.
The main goal of public health is to create a rational public health service with a high efficiency. Therefore, research related to improving the work of health care bodies and institutions, the scientific organization of work of medical personnel, etc. is of particular importance to it. The topics of such research may include: assessing the nature and volume of the population’s needs for medical care; research into the influence of various factors that determine these needs; assessing the effectiveness of the existing health care system; developing ways and means to improve it; drawing up forecasts for the provision of medical care to the population.
2. Basics of medical statistics
2.1 Statistics. Subject and methods of research. Medical statistics
The word “statistics” comes from the Latin word “status” - state, position. For the first time this word was used in the middle of the 18th century by the German scientist Achenwal when describing the state of the state (German: Statistik, from Italian: stato - state).
Statistics:
1) type of practical activity aimed at collecting, processing, analysis and publication statistical information characterizing the quantitative patterns of social life (economics, culture, politics, etc.).
2) a branch of knowledge (and corresponding academic disciplines), which sets out general issues of collecting, measuring and analyzing mass quantitative data.
Statistics as a science includes sections: general theory of statistics, economic statistics, industry statistics, etc.
The general theory of statistics sets out general principles and methods of statistical science.
Economic statistics studies the national economy as a whole using statistical methods.
Industry statisticians study various sectors of the national economy using statistical methods (branches of statistics: industrial, trade, judicial, demographic, medical, etc.)
Like every science, statistics has its own subject of study– mass phenomena and processes public life, their research methods– statistical, mathematical, develops systems and subsystems of indicators that reflect the dimensions and qualitative relationships of social phenomena.
Statistics studies the quantitative levels and relationships of social life in inextricable connection with their qualitative side. Mathematics also studies the quantitative side of the phenomena of the surrounding world, but abstractly, without connection with the quality of these bodies and phenomena.
Statistics originated from mathematics and is widely used mathematical methods. This is a selective research method based on the mathematical theory of probability and the law large numbers, various methods for processing variation and time series, measuring correlations between phenomena, etc.
Statistics develops and special methodology for research and processing of materials: mass statistical observations, method of groupings, average values, indices, method of graphic images.
In the literature, as a rule, there is no distinction between mathematical and statistical methods used in statistics.
The main task of statistics, like any other science, is to establish the patterns of the phenomena being studied.
One of the branches of statistics is medical statistics, which studies the quantitative side of mass phenomena and processes in medicine.
Health statistics studies the health of society as a whole and its individual groups, establishes the dependence of health on various factors of the social environment.
Health statistics analyzes data on medical institutions, their activities, evaluates the effectiveness of various organizational measures for the prevention and treatment of diseases.
The requirements for statistical data can be formulated in the following provisions:
1) reliability and accuracy of materials;
2) completeness, understood as coverage of all objects of observation for the entire study period, and obtaining all information on each object in accordance with the established program;
3) comparability and comparability, achieved in the process of observation by the unity of the program and nomenclatures and in the process of data processing and analysis - by the use of unified methodological techniques and indicators;
4) urgency and timeliness of receiving, processing and submitting statistical materials.
The object of any statistical research is statistical population– a group or set of relatively homogeneous elements, i.e. units taken together within specific boundaries of time and space and possessing signs of similarity and difference
The purpose of studying any statistical population is to identify common properties, general patterns of various phenomena, since these properties cannot be detected by analyzing individual phenomena.
A statistical population consists of units of observation. Unit of observation– each primary element of a statistical population endowed with signs of similarity. For example: a resident of the city N., born in a given year, fell ill with the flu, etc.
Signs of similarity serve as the basis for combining units of observation into a population. The volume of the statistical population is the total number of observation units.
Accounting characteristics– characteristics by which units of observation are distinguished in a statistical population.
Signs of similarity serve as the basis for combining units into a set; signs of difference, called accounting features, are the subject of their special analysis
In my own way accounting characteristics may be:
– qualitative (they are also called attributive): they are expressed verbally and have a defining character (for example, gender, profession);
– quantitative, expressed as a number (for example, age).
According to their role in the aggregate, accounting characteristics are divided:
– factorial, which influence changes in the characteristics that depend on them;
– effective, which depend on factor ones.
Distinguish two types of statistical population:
– general consisting of all units of observation that can be attributed to it depending on the purpose of the study;
– selective– part of the general population selected by a special sampling method.
Each statistical aggregate depending on the purpose of the study, can be considered both general and selective. The sample population must be representative in quantity and quality in relation to the general population.
Representativeness– representativeness of the sample population in relation to the general population.
Representativeness is quantitative– sufficient number of observation units in the sample population (calculated using a special formula).
Representativeness is qualitative– correspondence (sameness) of characteristics characterizing the units of observation of the sample population in relation to the general population. In other words, the sample population should be as close as possible to the general population in terms of qualitative characteristics.
Representativeness is achieved by correctly selecting observation units, in which any unit of the entire population as a whole would have an equal opportunity to be included in the sample population.
The sampling method is used in cases where it is necessary to conduct an in-depth study, while saving effort, money, and time. The sampling method, when applied correctly, gives fairly accurate results suitable for use for practical and scientific purposes.
There are a number of methods for selecting units for a sample population, of which the following methods are most often used: random, mechanical, typological, serial, cohort.
Random selection is characterized by the fact that all units of the general population have equal opportunities to be included in the sample (by lot, according to a table of random numbers).
Mechanical selection is characterized by the fact that from the entire (general) population a mechanically selected, for example, every fifth (20%) or every tenth (10%) observation unit is taken.
Typological selection (typical sampling) allows you to select observation units from typical groups of the entire population. To do this, first, within the general population, all units are grouped according to some characteristic into typical groups (for example, by age). From each such group a selection is made (random or mechanical method).
Serial selection is similar to typological selection, i.e. First, within the general population, all units are grouped according to some characteristic into typical groups (for example, by age), and then, in contrast to typological selection, several groups (series) are taken as a whole.
The cohort selection method is characterized by the fact that all units of the population selected for the study are united by a common feature (for example, year of birth, year of marriage registration). This selection method is often used in demographic studies. The observation period, in this case, must be at least 5 years.
Stages of statistical research. Statistical research is based on certain principles, rules and techniques developed over many years of practice and scientifically generalized, which together constitute statistical methodology.
Statistical work in healthcare practice and special medical research consists of four successive stages, which in turn are divided into a number of static operations:
1st stage – drawing up a research plan and program (preparatory work). Determining the purpose and objectives of the study.
Drawing up an observation plan and program:
– determination of the object of observation;
– establishment of a unit of observation;
– determination of accounting characteristics;
– drawing up or choosing the form of an accounting document;
– definition of type and method statistical observation.
Drawing up a materials summary program:
– establishment of grouping principles;
– identification of grouping characteristics;
– determination of the necessary combinations of features;
– drawing up layouts of statistical tables.
Drawing up an organizational research plan:
– determination of the place, time and subject of observation,
– summaries and processing of materials.
Elements of statistical tables:
1. The title of the table (clear, concise), which defines its content.
2. Statistical subject - as a rule, this is the main feature of the phenomenon being studied. It is usually located along the horizontal rows of the table.
3. Statistical predicate is a sign that characterizes the subject. Located in the vertical columns of the table.
4. Summary columns and rows – complete the design of the table.
Types of statistical tables
1. Simple is a table that presents only the quantitative characteristics of the subject (Table 2.1)
Table 2.1. Number of beds in hospitals in the city of N. as of 01/01/2003
Simple tables are easy to compile, but their information is of little use for analysis, so they are used mainly for statistical reporting (information about the network and activities of medical institutions, etc.). 2. Group is a table that presents the connection of the subject with only one of the signs of the predicate (Table 2.2). Table 2.2. Distribution of patients by gender and age treated in various departments of the hospital in the city of N. in 2002.
Branch name Age groups (years) Total Both sexes Total Therapeutic Surgical Gynecological Total A group table can contain an unlimited number of attributes in the predicate (no more than 24 are recommended, since such tables are not convenient to work with), but they are combined with the subject only in pairs: – hospital and patients treated by gender, – hospital and patients treated by age. 3. Combination is called a table whose data characterizes the connection of the subject with a combination of features of the predicate (Table 2.3). Table 2.3. Distribution of patients treated in hospital No. 4 of the city of A., by nosological forms, gender and age for 1997–2002.
Combination tables are used to conduct a detailed study of the relationships between individual characteristics of a phenomenon, or between several homogeneous phenomena that differ in only one characteristic. 2nd stage– statistical observation (registration). Briefing. Providing registration forms. Collection of material. Registration quality control. 3rd stage– statistical summary and grouping of materials. Counting and logical verification of materials. Marking (encryption) of materials according to grouping characteristics. Calculating totals and filling out tables. Counting processing and analysis of materials: – calculation of relative values (statistical coefficients), calculation of average values; – compilation of time series; – statistical assessment of the reliability of sample indicators and testing of hypotheses; – construction of graphic images; – measuring the connection between phenomena (correlation); – attraction of comparative data. Stage 4– analysis, conclusions, proposals, implementation of research results into practice. Statistical research is not necessarily scientific work; in the daily practice of healthcare institutions, all of the listed stages are carried out. Thus, the practice of filling out accounting documents corresponds to the stage of statistical observation; preparation of periodic reports - the stage of statistical summary and grouping of materials; the analysis stage consists of the text part of the reports, the compilation of explanatory notes and opportunistic reviews that provide a scientific and medical interpretation and explanation of digital data. In this case, the first stage of statistical research corresponds to the development of a system for accounting and reporting of healthcare institutions. 2.2 Relative values Derived value - an indicator obtained as a result of transformation absolute value based on its comparison with another absolute value. It is expressed as a ratio or difference in absolute values. The main types of derived quantities used in biomedical statistics are relative values (statistical coefficients) and average values. Absolute values characterize, for example, population size, number of births, isolated cases of certain infectious diseases, and their chronological fluctuations. They are necessary for organizational planning in healthcare (for example, planning the required number of beds), as well as for calculating derived values. However, in the overwhelming majority of cases, series of absolute numbers are not suitable for comparison, identifying connections and patterns, and qualitative features of the processes being studied. Therefore, they calculate relative values, types, which depend on what is being compared: – a phenomenon with the environment from which it originates; – constituent elements of the same phenomenon; – independent phenomena that are compared with each other. The following types of relative quantities are distinguished: – Intensive coefficients (relative frequency values). – Extensive coefficients (relative values of distribution or structure). – Coefficients (relative values) of the relationship. – Coefficients (relative values) of visibility. Intensive coefficients– characterize the strength, frequency (degree of intensity, level) of the distribution of a phenomenon in the environment in which it occurs, with which it is directly related. Intensive indicator = – ·
100 (1000; 10000... etc.) Calculation of intensive indicators is done as follows. For example: the population of the N region in 2003 was 1318.6 thousand people. During the year, 22.944 thousand people died. To calculate the mortality rate, it is necessary to compose and solve the following proportion: 1.318.600 – 22.944 22.944 ·
1000 1000 – X X = – = 17.4 ‰. Conclusion: the mortality rate in 2003 was 17.4 per 1000 population. It should be remembered that when calculating intensive coefficients we are always dealing with two independent, qualitatively different aggregates, one of which characterizes the environment, and the second - the phenomenon (population and number of births; number of sick and number of deaths). It cannot be considered that the sick are “divided into those who have recovered and those who have died”; the dead are a new (in this case irreversible) phenomenon, an independent group. Examples of using intensive coefficients: – determination of the level, frequency, prevalence of a particular phenomenon; – comparison of a number of different populations according to the degree of frequency of a particular phenomenon (for example, comparison of birth rates in different countries, comparison of mortality rates in different age groups); – identifying the dynamics of changes in the frequency of a phenomenon in the observed population (for example, changes in the prevalence of infectious diseases in the country’s population over several years). Ratio coefficients– characterize the numerical ratio of two independent aggregates that are not directly related to each other, comparable only logically, according to their content. The technique for calculating ratio indicators is similar to the technique for calculating intensive indicators: Ratio indicator = – ·
1; 100 (1000; 10000, etc.) Phenomenon B Ratio coefficients usually indicate the numerical ratio of two phenomena that are not directly related to each other. Calculation of ratio indicators is done as follows. For example: the number of children in the N region in 2004 was 211,480 people. The number of pediatricians in the region in 2004 was 471. To calculate the supply of pediatricians to the child population, it is necessary to compile and solve the following proportion: 211.489
– 471
471 ·
10.000 10.000 – X X = – = 22.3 Conclusion: The supply of pediatricians to the child population was 22.3 per 10,000 children. Extensive coefficients can be used to characterize the structure of the birth rate (distribution of births by gender, height, weight); structure of mortality (distribution of deaths by age, gender and causes of death); structure of morbidity (distribution of patients by nosological forms); composition of the population by gender, age and social groups, etc. Calculation of extensive coefficients is done as follows. For example: in 2003, the population of the N region was 1318.6 thousand people, including 605.3 thousand men. If we take the entire population of the N region as 100%, then the proportion of men will be: 1.318.600 – 100% 605.300 ·
100 605.300 – Х Х = – = 45.9% Conclusion: the share of the male population of the N region in 2003 was 45.9% A characteristic feature of extensive coefficients is their interconnectedness, causing a certain automaticity of shifts, since their sum is always 100%. For example, when studying the structure of morbidity, the proportion of a particular disease may increase in the following cases: 1) with its true growth, i.e. with an increase in the intensive indicator; 2) at the same level, if the number of other diseases during this period decreased; 3) when the level of a given disease decreases, if the decrease in the number of other diseases occurred at a faster pace. Extensive coefficients give an idea of the share of a particular disease (or class of diseases) only in a given population group and only for a certain period. Visibility factors– are used for the purpose of more visual and accessible comparison of series of absolute, relative or average values. They represent a technical technique for converting digital indicators. This coefficient is obtained by transforming a number of quantities in relation to one of them - basic(any, not necessarily initial). This basic value is taken as 1; 100; 1000, etc., and the remaining values of the series, using the usual proportion, are recalculated in relation to it (Table 2.4). Table 2.4. Birth rate in Russia for 1997 and 2000. (per 1000 people)
Visualization coefficients can be used to demonstrate trends in dynamic shifts and changes in the process under study (increasing or decreasing).
Nosological
forms
Age (in years)
Total
Up to 30
31 – 40
41 – 50
over 50
Pneumonia
M
AND
OP
M
AND
OP
M
AND
OP
M
AND
OP
M
AND
OP
Bronchitis
Tracheitis
Flu
ARVI
Total
Phenomenon
Event A
STATE BUDGET EDUCATIONAL INSTITUTION
HIGHER PROFESSIONAL EDUCATION
“KRASNOYARSK STATE MEDICAL UNIVERSITY named after Professor V.F. Voino-Yasenetsky"
MINISTRY OF HEALTH OF THE RUSSIAN FEDERATION
College of Pharmacy
Specialty 060501 Nursing
Qualification Nurse
TO THEORETICAL LESSONS
In the discipline "Public health and healthcare"
Agreed at a meeting of the Central Committee
Protocol number…………….
"___"____________ 2015
Chairman of the Central Medical Committee Nursing
………………Cheremisina A.A.
Compiled by:
………… Korman Y.V.
Krasnoyarsk 2015
Lecture 1
Subject. 1.1. Public health and public health as a scientific discipline
Lecture outline:
1. Public health and healthcare as a scientific discipline about the patterns of public health, the impact of social conditions and environmental factors, lifestyle on health, ways to protect and improve it.
2. Problems of social policy in the country. Fundamentals of domestic health care policy. Legislative framework of the industry. Health care problems in the most important socio-political and government documents (Constitution of the Russian Federation, Legislative acts, decisions, regulations, etc.).
3. Healthcare as a system of measures to preserve, strengthen and restore the health of the population. Main directions of health care reform.
Information block:
Public health and healthcare as a scientific discipline about the patterns of public health, the impact of social conditions and environmental factors, lifestyle on health, ways to protect and improve it. The relationship between the social and the biological in medicine. Basic theoretical concepts of medicine and healthcare.
The role of the discipline “Public Health and Healthcare” in the practical activities of a dentist, healthcare authorities and institutions, in planning, management, and organization of work in healthcare. The main methods of research in the discipline: statistical, historical, experimental, sociological, economic-mathematical, modeling, method of expert assessments, epidemiological, etc.
The emergence and development of social hygiene and health care organization (public medicine) in foreign countries and in Russia.
Problems of social policy in the country. Fundamentals of domestic health care policy. Legislative framework of the industry. Health care problems in the most important socio-political and government documents (Constitution of the Russian Federation, Legislative acts, decisions, regulations, etc.). Healthcare as a system of measures to preserve, strengthen and restore the health of the population. Main directions of health care reform.
Theoretical aspects of medical ethics and medical deontology. Ethical and deontological traditions of domestic medicine. Bioethics in the activities of a dentist: the procedure for using new methods of prevention, diagnosis and treatment, conducting biomedical research, etc.
Health as an object of the health service.
Health levels:
1. The health of an individual is individual.
2. The health of groups of people is collective.
Health of small groups (social, ethnic, professional background).
The health of the population by belonging to the administrative-territorial unit (population of the city, village, district).
Public health - the health of society, the population as a whole (national, global scale).
1. Definition of the concept - individual health.
The Constitution of the World Health Organization (WHO) includes a definition of health as a state of complete physical, spiritual and social well-being, and not just the absence of disease or infirmity.
For practical use, we will use the definition of health as a human condition that has physical, psychological and social parameters, each of which can be represented as a continuum with positive and negative poles.
Positive pole ( good health) is characterized by the ability to withstand the effects of adverse factors, and the negative pole (poor health) is characterized by morbidity and mortality.
Individual health is assessed by subjective (well-being, self-esteem) and objective (deviation from the norm, severe heredity, presence of genetic risk, reserve capabilities, physical and mental condition) criteria.
In a comprehensive assessment of individual health, the population is divided into health groups:
Group 1 - healthy individuals (who have not been sick for a year or who rarely see a doctor without losing their ability to work);
Group 2 - practically healthy individuals with functional and some morphological changes or who were rarely ill during the year (isolated cases of acute diseases);
Group 3 - patients with frequent acute diseases (more than 4 cases and 40 days of disability per year);
Group 4 - patients with long-term chronic diseases (compensated state);
Group 5 - patients with exacerbation of long-term diseases (subcompensated state).
2. Definition of the concept – public health.
Definitions given by the Ministry of Health of the Russian Federation:
Public health is a medical and social resource and potential of society that contributes to ensuring national security.
Population health is a medical, demographic and social category that reflects the physical, mental, and social well-being of people carrying out their life activities within certain social communities.
The basis for assessing the state of public health is accounting and analysis of:
Number of cases of diseases, injuries and poisonings detected for the first time or aggravated cases of chronic pathology;
The number of disabled people newly identified and registered in total;
Numbers of deaths;
Physical development data.
3. Factors determining public health.
Risk factors are potentially hazardous to health factors of a behavioral, biological, genetic, environmental, social, environmental and work environment that increase the likelihood of developing diseases, their progression and unfavorable outcome.
In contrast to the direct causes of the occurrence and development of diseases, risk factors create an unfavorable background, i.e. contribute to the occurrence and development of the disease. However, it should be borne in mind that these categories are closely interrelated with each other.
Yu.P. Lisitsin (1989) determined that the influence of factors determining health correlates in the following proportion:
Lifestyle accounts for 50-55%;
For internal hereditary-biological factors (predisposition to hereditary diseases) - 18-22%;
Environmental factors (air, water, soil pollution with carcinogenic and other harmful substances, sudden changes in atmospheric phenomena, radiation, geographical location locality) - 17-20%;
Level of development of health care (providing the population with medicines, quality and timeliness of medical care, development logistics bases, carrying out preventive measures) - 8-12 percent.
3.1. Lifestyle is the main factor determining health.
Lifestyle is qualified as a system of the most essential, typical characteristics of the way of activity or activity of people, in the unity of its quantitative and qualitative aspects, which are a reflection of the level of development of productive forces and production relations.
Lifestyle generalizes and includes four categories: economic – “standard of living”, sociological – “quality of life”, socio-psychological – “lifestyle” and socio-economic – “way of life”.
1. Lifestyle is the conditions in which people’s life activities take place (social and cultural life, everyday life, work).
2.Lifestyle - individual characteristics behavior, manifestations of life, activity, image and style of thinking.
3. Standard of living - characterizes the size and structure of a person’s material needs (quantitative category).
4. Quality of life (QOL) is a multidimensional concept at its core, multifactorial and in a broad sense defined as the degree of possibility of realizing a person’s material and spiritual needs.
According to the definition of the Ministry of Health of the Russian Federation, quality of life is a category that includes a combination of life support conditions and health conditions that allow one to achieve physical, mental and social well-being and self-realization.
WHO definition (1999): Quality of life is the optimal state and degree of perception by individuals and the population as a whole of how their needs (physical, emotional, social, etc.) are met and opportunities are provided to achieve well-being and self-realization.
F KSMU 4/3-04/03
Karaganda State Medical University
Department of Social Medicine and Health OrganizationLECTURE
Topic: “Public health and healthcare as a science and subject of teaching”
Discipline "Public health and healthcare"
Specialty 5B110400 - “Medical and preventive care”
Time -1 hour
Karaganda 2014
Approved at a department meeting
_________ 2014 Protocol No. ____
Head department, candidate of medical sciences, associate professor A.K. Sultanov
Topic: “Public health and healthcare as a science and subject of teaching. Methods for studying and assessing public health"
Lecture outline
Health levels
Risk factors, groups, concept
Methodology and methods of public health and healthcare research
Public health, as a medical specialty and the science of public health
Stages of healthcare development.
Relevance of the subject public health
The term “recreation” is even less commonly used in medical literature, i.e. a set of preventive, therapeutic and health measures aimed at preserving the health of healthy people. People's health, its criteria, ways to preserve and strengthen it in difficult socio-economic conditions have almost completely fallen out of the sphere of interests of modern medicine and healthcare in Kazakhstan. In this regard, before talking about public health, it is necessary to define the term “health” and identify the place of public health in this hierarchy.
2. Health levels
Methodology and methods for researching public health and healthcare So, the World Health Organization (WHO) back in 1948. formulated that “health is a state of complete physical, spiritual and social well-being, and not just the absence of disease and physical defects.” WHO has proclaimed the principle that “the enjoyment of the highest attainable standard of health is a fundamental right of every person.” It is customary to distinguish 4 levels of health study:
Level 1 – individual health.
Level 2 – health of small or ethnic groups – group health.
Level 3 – public health, i.e. people living in a specific administrative-territorial unit (region, city, district, etc.).
Level 4 – public health – the health of society, the population of a country, continent, world, population as a whole.
Public health and healthcare, as an independent medical science, studies the impact of social factors and environmental conditions on the health of the population in order to develop preventive services. Public health and healthcare studies a wide range of different medical aspects, sociological, economic, managerial, and philosophical problems in the field of public health in a specific historical setting.
The following definition of the concept was developed: “Public health is the most important economic social potential of the country, determined by the influence of various environmental factors and lifestyle of the population, allowing to ensure an optimal level of quality and safety of life.”
Unlike various clinical disciplines, public health studies the health status not of individual individuals, but of groups, social groups and society as a whole in connection with conditions and lifestyle. At the same time, living conditions and production relations, as a rule, are decisive for the state - economic revolutions and evolutionary periods, the cultural revolution bring the greatest benefits to society, but at the same time they can have negative impacts on his health. Greatest discoveries modernity in the field of physics, chemistry, biology, urbanization of the population in the 20th century, rapid development of industry in many countries, large volumes of construction, chemicalization of rural ecology, which has a detrimental effect, first of all, on the health of the population, causing certain diseases that sometimes in their prevalence they acquire an epidemiological character.
Antagonistic contradictions between scientific and technological progress and the state of public health in our country arise due to the state’s underestimation of preventive measures. Consequently, one of the tasks of our science is to reveal such contradictions and develop recommendations for the prevention of negative phenomena and factors that negatively affect the health of society.
For the planned development of the national economy, information on the population size and the determination of its forecasts for the future are of great importance. Public health identifies patterns of population development, studying demographic processes, predicts the future, and develops recommendations for state regulation of population size.
Thus, public health is characterized by the simultaneous complex impact of social, behavioral, biological, geophysical and other factors. Many of these factors can be identified as risk factors. What are disease risk factors?
3. Risk factors, groups, concept
– potentially hazardous to health factors of a behavioral, biological, genetic, environmental, social nature, environmental and industrial environment, increasing the likelihood of developing diseases, their progression and unfavorable outcome.
Unlike the direct causes of diseases (bacteria, viruses, deficiency or excess of any microelements, etc.), risk factors act indirectly, creating an unfavorable background for the occurrence and further development diseases.
When studying public health, the factors that determine it are usually combined into the following groups:
Socio-economic factors(working conditions, living conditions, material well-being, level and quality of nutrition, rest, etc.).
Socio-biological factors(age, gender, predisposition to hereditary diseases, etc.).
Environmental and climatic factors(habitat pollution, average annual temperature, the presence of extreme natural and climatic factors, etc.).
Organizational or medical factors(provision of the population with medical care, quality of medical care, availability of medical and social care, etc.).
At the same time, the division of factors into certain groups is very arbitrary, since the population is exposed to the complex influence of many factors, in addition, factors influencing health interact with each other, change in time and space, which must be taken into account when carrying out comprehensive medical social research.
The second part of the science of public health and healthcare includes the development of scientifically based, most optimal methods of healthcare management, new forms and methods of operation of various medical institutions, ways to improve the quality of medical care, and substantiates optimal solutions to economic and managerial problems in healthcare.
The rapid growth in the development of medical science has armed doctors with new, modern methods for diagnosing complex diseases and effective means of treatment. All this simultaneously requires the development of new organizational forms and conditions for the activities of doctors, health care facilities, and sometimes the creation of completely new, previously non-existent medical institutions. There is a need to change the management system of medical institutions and the placement of medical personnel; there is a need for revision regulatory framework healthcare, expanding the independence of heads of medical institutions and the rights of doctors.
As a consequence of all of the above, conditions are being created for revising options for more optimal solutions to economic problems of healthcare, introducing elements of intradepartmental economic accounting, economic incentives for the quality work of medical personnel, etc.
These problems determine the place and importance of science in the further improvement of domestic healthcare.
The unity of theory and practice of domestic health care is expressed in the unity of theoretical and practical tasks, methodological techniques of domestic public health and healthcare.
Thus, of leading importance in science is the question of studying the effectiveness of the impact on the health of the population of all activities carried out by the state and the role of health care and individual medical institutions in this, both with state and non-state forms of ownership, i.e. the subject reveals the significance of the entire diversity of the country’s socio-economic life and determines ways to improve medical care for the population.
4. Methodology and methods for researching public health and healthcare Public health and healthcare have their own methodology and research methods. Such methods are: statistical, historical, economic, experimental, timing research, sociological methods, etc.
Statistical method is widely used in most studies: it allows you to objectively determine the level of health of the population, as well as the efficiency and quality of work of medical institutions.
Historical method allows the study to trace the state of the problem being studied at different historical stages of the country's development.
Economic method makes it possible to establish the influence of the economy on healthcare and healthcare on the state’s economy, to determine the most optimal ways to use public funds to effectively protect the health of the population. Planning issues financial activities health authorities and medical institutions, the most rational use Money, assessment of the effectiveness of health care actions to improve the health of the population and the impact of these actions on the country’s economy - all this constitutes the subject of economic research in the field of health care.
Experimental method include setting up various experiments to find new, most rational forms and methods of operation of medical institutions and individual health services.
It should be noted that most studies predominantly use a complex methodology using most of these methods. So, if the task is to study the level and state of outpatient care to the population and determine ways to improve it, then the morbidity of the population, the number of visits to outpatient clinics are studied using the statistical method, its level in different periods and its dynamics are analyzed historically. The proposed new forms in the work of polyclinics are analyzed using the experimental method: their economic feasibility and effectiveness are checked.
Methods may be used in the study timing studies(timing of the work of medical personnel, study and analysis of time spent by patients receiving medical care, etc.).
Sociological methods are often used (interviewing methods, questionnaire methods), which makes it possible to obtain a generalized opinion of a group of people about the object (process) of study.
The source of information is mainly state reporting documentation of treatment and preventive medical institutions; for a more in-depth study, the collection of material can be carried out on specially designed cards, questionnaires, which include all the questions to obtain the necessary information in accordance with the approved research program and the tasks assigned to the researcher. For this purpose, the researcher can, using a special program, enter the necessary data into the computer from the primary registration documents.
The vast majority of socio-hygienic studies of group health, population health and public health in previous years dealt with the quantitative assessment of health. True, with the help of indicators, indices and coefficients, scientific research has always tried to assess the quality of life. The term “quality of life” itself has begun to be used in the domestic scientific literature in the last 10-15 years. This is understandable; only then can we talk about the “quality of life” of the population when in a country (as has long happened in the developed countries of Europe, America, Japan and some others) basic material and social benefits are available to the majority of the population.
According to WHO definition (1999), the quality of life– the optimal state and degree of perception by individuals and the population as a whole of how their needs (physical, emotional, social, etc.) are met and opportunities are provided to achieve well-being and self-realization.
In our country, quality of life most often means a category that includes a combination of life support conditions and health conditions that allow one to achieve physical, mental, social well-being and self-realization.
Despite the absence of a globally accepted concept of “quality of health” as the most important component of “quality of life,” attempts are being made to give a comprehensive assessment of public health (quantitative and qualitative).
Basic theoretical and organizational principles
The concept of “healthcare” means activities to preserve, improve, ensure and strengthen the health of various population groups. The main legislative acts enshrine the human right to protection and promotion of health. Optimization of the healthcare system is the most important part of the state’s socio-economic policy. Healthcare is seen as government system with unity of goals, interaction and continuity of services (therapeutic and preventive), universal availability of qualified medical care, and a real humanistic orientation.
Priority structural element The healthcare system is the preventive activities of medical workers, the development of medical and social activity and attitudes towards a healthy lifestyle among various groups of the population.
The main direction in the development and improvement of healthcare at the present stage is the protection of motherhood and childhood, the creation of optimal socio-economic, legal and medical-social conditions for improving the health of women and children, family planning, and solving medical and demographic problems.
The public nature of health care ensures funding, training and improvement of personnel. The activities of bodies and institutions are carried out on the basis of state legislation and regulatory documents. The principle of unity of medical science and practice is implemented in the form of joint activities and the introduction of scientific developments in healthcare institutions.
The most important theoretical problems of health care include: the social conditionality of public health, disease as a biosocial phenomenon, the main categories of health care (public health, material and economic base, personnel, etc.), forms and ways of development of health care under various socio-economic conditions and etc.
The World Health Organization has defined 4 categories of general indicators that characterize the state of health care in a country: 1) indicators related to health policy; 2) social and economic indicators; 3) indicators of the provision of medical and social assistance; 4) indicators of the health status of the population.
The founders of domestic social medicine defined social medicine as the science of public health and healthcare. Its main task is to study the influence of medical and social factors, conditions and lifestyle on the health of various population groups, to develop scientifically based recommendations for the prevention and elimination of unfavorable social conditions and factors, as well as health measures to improve the level of public health. The main purpose of social medicine and health care management as a science and academic discipline is to evaluate the criteria of public health and the quality of medical care and their optimization.
Subject structure: 1) history of health care; 2) theoretical problems of health care; 3) health status and methods of studying it; 4) organization of medical and social security and health insurance; 5) organization of medical care to the population; 6) ensuring the sanitary and epidemiological well-being of the population; 7) economic and planning-organizational forms of improving healthcare, management, marketing and modeling of medical services; 8) the international cooperation in the field of medicine and healthcare.
Methods of medical and social research: 1) historical;
2) dynamic observation and description; 3) sanitary-statistical; 4) medical and sociological analysis; 5) expert assessments; 6) system analysis and modeling; 7) organizational experiment; 8) planning and normative, etc.
Social medicine is the science of health care strategy and tactics. The objects of medical and social research are:
1) groups of persons, population of the administrative territory; 2) individual institutions (clinics, hospitals, diagnostic centers, specialized services); 3) health authorities; 4) environmental objects; 5) general and specific risk factors for various diseases, etc.
Stages of healthcare development
The training of medical personnel was carried out in medical-surgical schools (since 1786), and since 1798 - in the St. Petersburg and Moscow medical-surgical academies. In 1755, the first Moscow University in Russia with a medical faculty was created.
An outstanding contribution to health protection was made by M. V. Lomonosov, who in his work “The Word on Reproduction and Preservation Russian people"gave an in-depth analysis of healthcare and proposed a number of specific measures to improve its organization.
In the first half of the 19th century. the first scientific medical schools are formed: anatomical (P. A. Zagorsky), surgical
(I. F. Bush, E. O. Mukhin, I. V. Buyalsky), therapeutic
(M. Ya. Mudrov, I. E. Dyadkovsky). N. I. Pirogov \
From the second half of the 19th century V. In addition to government agencies, public medicine was also involved in health issues: the Society for the Protection of Public Health (1878),
through the organizational forms of public medicine (medical periodicals, medical societies, congresses, commissions), the first local system of medical care in Russia (county doctors) was created, and the beginning of the organization of sanitary affairs in St. Petersburg was laid (1882),
In the 70s of the 20th century, hygiene was formed as an independent discipline, the first scientific hygiene schools were created (A.P. Dobroslavin, F.F. Erisman).
For the first time in Russia (together with sanitary doctors A.V. Pogozhev and E.M. Dementiev), a comprehensive social and hygienic study of factories and factories in the Moscow province (1879-1885) was carried out.
The first sanitary doctors I. I. Molleson, I. A. Dmitriev, G. I. Arkhangelsky, E. A. Osipov, N. I. Tezyakov, Z. G. Frenkel and others did a lot for the development of zemstvo and city sanitary organizations.
I. I. Molleson, the first sanitary doctor in Russia, created the first medical and sanitary council - a collegial body designed to manage zemstvo medicine. He proposed a project for organizing medical stations in rural areas, the position of a district sanitary doctor to study the sanitary condition of the population, working and living conditions, the causes of diseases and the fight against them. Organizer and leader of more than 20 provincial congresses of zemstvo doctors. I. I. Molleson emphasized: “Social medicine as a branch of knowledge and activity is broad and covers ... all activities that can improve the living conditions of the masses of the population.”
E. A. Osipov is one of the founders of zemstvo medicine and sanitary statistics. For the first time in Russia, he introduced card registration of diseases. Created the zemstvo Moscow provincial sanitary organization (1884). He developed the principle of operation of a medical district with a hospital-hospital, the functions of a rural doctor, as well as a program for sanitary inspection of the province.
N. A. Semashko - theorist and organizer of health care, the first people's commissar of health care (1918-1930). Under his leadership, the principles of healthcare were developed - state character, preventive orientation, free and generally accessible qualified medical care, unity of science and practice, broad public participation in solving health issues. N. A. Semashko created a new science - social hygiene and became the first head of the department of social hygiene (1922). He created new types of healthcare - maternal and infant health care, sanatorium and resort business. With his active participation, the State Scientific Institute of Public Health named after. L. Pasteur, the system of higher education was rebuilt medical education, institutes of physical culture were organized in Moscow and Leningrad.
Z. P. Solovyov - theorist and organizer of civil and military health care, deputy people's commissar Health, Head of the Main Military Sanitary Directorate. In 1923 he organized the Department of Social Hygiene at the 2nd Moscow Medical Institute. Contributed huge contribution in the development of preventive health care, in the reform of medical education.
Z. G. Frenkel is one of the founders of social hygiene in the country. Organizer and head of the department of social hygiene of the 2nd Leningrad Medical Institute (1923-1949), a major specialist in municipal hygiene, demography and gerontology, head of the Hygienic Society of Leningrad for 27 years.
The period of the Great Patriotic War and post-war years related to development military medicine, restoration of the material base of healthcare and active training of medical personnel.
Since 1961, a number of legislative acts and resolutions of the Union Government have been adopted aimed at developing the healthcare system. The protection of public health has been declared the most important social task. The material base of health care is being strengthened, medical care is being specialized, and the primary health care system is being improved. In 1978, a WHO conference was held in Almaty on the organization of primary health care for the population, at which there were 146 participating countries. The Magna Carta developed at this conference formed the basis of new thinking about the health of nations and divided the history of healthcare organization into before and after Alma-Ata. The greatest merit in organizing and holding the conference, and in the development of healthcare in the Republic of Kazakhstan belongs to the first academician of medicine of Kazakhstan T.Sh. Sharmanov. Laureate of international prizes and awards, founder and director of the National Research Institute of Nutrition T.Sh. Sharmanov continues to produce new medical knowledge and technologies today.
The formation of social hygiene in these years was facilitated by famous scientists S.V. Kurashev, G.A. Batkis, S.Ya. Freidlin, E.Ya. Belitskaya and others Modern period medical and social research into problems of public health and healthcare is associated with the names of such scientists as: Yu. P. Lisitsyn, O. P. Shchepin, I. N. Denisov, Kucherenko, I. V. Lebedeva, V. A. Minyaev, A. M. Moskvichev, etc., in Russia, and in Kazakhstan O. Zhuzhanov. A.A.Akanov, T.I.Slazhneva and others.
In recent years, the priority health problems have been such as maternal and child protection, the establishment of state sanitary supervision and environmental protection, medical care in the context of a new economic mechanism, market economy and health insurance, introducing the principles of family medicine, improving the training of medical personnel
Illustrative material:
Slides:
Table layouts.
Literature:
1.Yu.P. Lisitsin, N.V. Polunina “Public health and healthcare” M: Medicine, 2002, pp. 353-357.
2. Current problems of social medicine and health care management. // In the collection: Selected lectures (edited by Doctor of Medical Sciences Kulzhanov M.K.). – Almaty, 1994. – 175 p.
3. Yuryev V.K., Kutsenko G.I. Public health and healthcare. – St. Petersburg, Petropolis. – 2000. – 914 p.
Literature
Additional:
1. Reshetnikov A.V., Shapovalova O.A. Health as a subject of study in the sociology of medicine: tutorial. - M., 2008. - 64 p.
Medic V.A. A Guide to Statistics in Medicine and Biology. 3 volumes Medic V.A., Tokmachev M.S., Fishman B.B., Komarov Yu.M. - Publisher: M.: Medicine, 2006. - 352
Akanov A.A., Devyatko N.V., Kulzhanov M.K. Public health in Kazakhstan: concept, problems and prospects. - Almaty, - 2001-100s.
In Kazakh language
main:
Bigalieva R.K., Ismailov Sh.M. Social medicine and health care management: Textbook (in Kazakh). - Almaty, 2001.- 371 p.
Control questions
Give the concept of “health”, “public health”
2.How many health levels are there?
What are risk factors?
What is the proportion of lifestyle factors on health?
5.What is the share of health care factors on health?
6. Basic methods of public health
What does public health study?
Basic methods for studying public health?
What are the main structures of the subject?
Healthcare system in the Republic of Kazakhstan
Ways to develop healthcare
Current state of healthcare in the Republic of Kazakhstan
Public health sector
Non-state health sector.
State program for the development of healthcare in the Republic of Kazakhstan
Page 1
Public health and healthcare as a science and subject of teaching.Basic methods of public health and public health science.
1 question. Public health and healthcare as a science and subject of teaching.
Public health and healthcare as an independent medical science studies the impact of social conditions and environmental factors on the health of the population in order to develop preventive measures to improve its health and improve medical care.
Unlike clinical disciplines, public health studies the health status not of individuals, but of groups, social groups and society as a whole in connection with conditions and lifestyle. In this case, living conditions and production relations, as a rule, are decisive.
Public health identifies patterns of population development, studies demographic processes, forecasts the future, and develops recommendations for state regulation of population size.
Of leading importance in the study of this discipline is the question of the effectiveness of the impact on the health of the population of measures carried out by the state, the role of healthcare and individual medical institutions in this.
Medicine is based on two basic concepts - “health” and “disease”. In modern literature there are a large number of definitions and approaches to the concept of “health”.
WHO definition: « Health is a state of complete physical, mental and social well-being, and not merely the absence of disease or infirmity.".
In medical and social research, when assessing health, it is advisable to distinguish four levels:
Level 1 - individual health - individual health;
Level 2 - health of social and ethnic groups - group health;
Level 3 - health of the population of administrative territories – regional health;
Level 4 - health of the population, society as a whole – public health.
According to WHO experts, in medical statistics, health at the individual level is understood as the absence of identified disorders and diseases, and at the population level - the process of reducing mortality, morbidity and disability, and increasing the perceived level of health.
Human health can be considered in various aspects: socio-biological, socio-political, economic, moral-aesthetic, psychophysical, etc. Therefore, terms that reflect only one facet of population health are now widely used - “mental health”, “reproductive health”, “general somatic health”, etc. Or - the health of a separate demographic or social group - “pregnant health”, “children’s health”, etc.
Currently, there are very few indicators that would objectively reflect the quantity, quality and composition of public health. The search and development of integral indicators and indices for assessing the health of the population is underway. WHO believes that these indicators should have the following qualities:
1. Availability of data. It must be possible to obtain the required data without carrying out complex special studies.
2. Comprehensiveness of coverage: The indicator must be derived from data covering the entire population for which it is intended.
3. Quality. National (or territorial) data should not vary over time and space in such a way that the indicator is significantly affected.
4. Versatility. If possible, the indicator should reflect a group of factors that are identified and influence the level of health.
5. Computability. The indicator should be calculated in the simplest and least expensive way possible.
6. Acceptability (interpretability): There must be acceptable methods for calculating the indicator and its interpretation.
7. Reproducibility. When using a health indicator by different specialists in different conditions and at different times, the results should be identical.
8. Specificity. An indicator should reflect changes only in those phenomena that it serves as an expression.
9. Sensitivity. The health indicator must be sensitive to changes in relevant phenomena.
10. Validity. An indicator must be a true expression of the factors of which it is a measure.
11. Representativeness. The indicator must be representative in reflecting changes in the health of population groups identified for management purposes.
12. Hierarchy. The indicator must be constructed according to a single principle for different hierarchical levels allocated in the population being studied for the diseases taken into account, their stages and consequences.
13. Goal consistency. The health indicator must adequately reflect the goals of maintaining and developing (improving) health and stimulate society to find the most effective ways to achieve these goals.
In medical and social research, it is traditional to use the following indicators to quantify group, regional and public health in Russia: 1. Demographic indicators. 2. Morbidity. 3. Disability. 4. Physical development.
1. Deduction of gross national product for health care.
2. Availability of primary health care.
3. Coverage of the population with medical care.
4. Level of immunization of the population.
5. The extent to which pregnant women are examined by qualified personnel.
6. Nutritional status of children.
7. Infant mortality rate.
8. Average life expectancy.
9. Hygienic literacy of the population.
From the point of view of the general classification of sciences, public health is on the border between natural science and social sciences, that is, it uses the methods and achievements of both groups. From the point of view of the classification of medical sciences, public health seeks to fill the gap between the groups of clinical (therapeutic) and preventive (hygienic) sciences. Public health provides a general picture of the state and dynamics of health and reproduction of the population and the factors determining them.
The methodological basis of public health as a science is the study and correct interpretation of the causes and connections between the state of public health and social relations.
Social and hygienic factors influencing public health include: working and living conditions, living conditions; salary level, culture and upbringing, nutrition, family relationships, quality and availability of medical care.
Public health is also influenced by climatic-geographical and hydrometeorological factors of the external environment.
A significant part of these conditions can be changed by society itself, and their impact on the health of the population can be both negative and positive.
Question 2. Public health methods.
1). Statistical method - the main method of social sciences. It allows you to establish and objectively evaluate changes in the health status of the population and determine the effectiveness of health care bodies and institutions; it is widely used in medical scientific research (hygienic, physiological, biochemical, clinical, etc.).
2). Expert assessment method serves as a complement to the statistical one. Its main task is to determine correction factors indirectly, because public health uses quantitative measurements using statistics and epidemiological methods. This allows forecasts to be made based on pre-formulated patterns, for example, forecasts of fertility, population, mortality, etc.
3). Historical method is based on the study and analysis of public health and healthcare processes at various stages of history. This is a descriptive method.
4). Economic research method makes it possible to establish the impact of the economy on healthcare and healthcare on the economy. For this purpose, methods used in economic sciences are used in the study and development of such issues as accounting, planning, financing, healthcare management, rational use of material resources, scientific organization of labor in healthcare bodies and institutions.
5). Experimental method is a method of searching for new, most rational forms and methods of work, creating models of medical care, introducing best practices, testing projects, hypotheses, creating experimental bases, medical centers, etc.
In public health, the experiment cannot be used often because of the administrative and legislative difficulties associated with it.
6). Simulation method develops in the field of healthcare organization, and consists of creating organizational models for experimental testing. Depending on the goals and problems, models vary significantly in scope and organization, and can be temporary or permanent.
7). Observation and survey method – used to supplement and deepen data using special research. For example, to obtain more complete data on the morbidity of persons in certain professions, they use the results obtained during medical examinations. To identify the nature and degree of influence of social and hygienic conditions on morbidity or mortality, survey methods (interviews, questionnaires) of individuals, families or groups can be used under a special program.
8). Epidemiological method. An important place among epidemiological research methods is occupied by epidemiological analysis, which is a set of methods for studying the characteristics of the epidemic process in order to determine the reasons contributing to the spread of this phenomenon in a given territory and to develop practical recommendations for its optimization. From the point of view of public health methodology, epidemiology is applied medical statistics, which in this case acts as the main, largely specific, method.
The use of epidemiological methods on large populations allows us to distinguish various components of epidemiology: clinical epidemiology, environmental epidemiology, epidemiology of non-communicable diseases, epidemiology of infectious diseases, etc. In public health, there are epidemiology of public health indicators.
Subject of science.
Items:
1. Public health.
2. Healthcare.
1. Public health
2. Healthcare
3.Risk factors
4. Lifestyle and conditions.
II. Natural and climatic.
IV. Psycho-emotional.
Objectives of science:
Sections of science:
Research methods used in public health and public health
Public health, like other scientific disciplines, has its own research methods.
1) Statistical method As a fundamental method of social science, it is widely used in the field of public health. It allows you to establish and objectively evaluate changes in the health status of the population and determine the effectiveness of the activities of health authorities and institutions. In addition, it is widely used in medical research (hygienic, physiological, biochemical, clinical, etc.).
2) Method of expert assessments serves as a complement to the statistical one, the main task of which is to determine indirectly certain correction factors.
Public health uses quantitative measurements using statistics and epidemiological methods. This makes it possible to make forecasts based on pre-formulated patterns, for example, it is quite possible to predict future fertility, population size, mortality, mortality from cancer, etc.
3) Historical method is based on the study and analysis of public health and healthcare processes at various stages of human history. The historical method is a descriptive, descriptive method.
4) Economic research method makes it possible to establish the influence of the economy on healthcare and, conversely, healthcare on the economy of society. Health economics is an integral part of a country's economy. Health care in any country has a certain material and technical base, which includes hospitals, clinics, dispensaries, institutes, clinics, etc. Sources of health care financing and issues of the most effective use of these funds are researched and analyzed.
To study the influence of socio-economic factors on people's health, methods used in economic sciences are used. These methods find direct application in the study and development of such health issues as accounting, planning, financing, health care management, rational use of material resources, scientific organization of labor in health care bodies and institutions.
5) Experimental method is a method of searching for new, most rational forms and methods of work, creating models of medical care, introducing best practices, testing projects, hypotheses, creating experimental bases, medical centers, etc.
Experiments can be carried out not only in natural sciences, but also in social sciences. In public health, the experiment may not be used often due to the administrative and legislative difficulties associated with it.
In the field of healthcare organization, a modeling method is being developed, which consists of creating organizational models for experimental testing. In connection with the experimental method, great reliance is placed on experimental zones and health centers, as well as on experimental programs on individual problems. Experimental zones and centers can be called “field laboratories” for conducting scientific research in the field of health. Depending on the goals and problems for which they were created, these models vary significantly in scope and organization, and can be temporary or permanent.
6) Method of observation and questioning. To replenish and deepen this data, special studies can be undertaken. For example, to obtain more in-depth data on the morbidity of people in certain professions, the results obtained during medical examinations of this contingent are used. To identify the nature and degree of influence of social and hygienic conditions on morbidity, mortality and physical development, survey methods (interviews, questionnaires) of individuals, families or groups of people can be used according to a special program.
Using the survey method (interview), you can obtain valuable information on a variety of issues: economic, social, demographic, etc.
7) Epidemiological method. Epidemiological analysis occupies an important place among epidemiological research methods. Epidemiological analysis is a set of methods for studying the characteristics of the epidemic process in order to determine the reasons contributing to the spread of this phenomenon in a given territory and to develop practical recommendations for its optimization. From the point of view of public health methodology, epidemiology is applied medical statistics, which in this case acts as the main, largely specific, method.
Time series.
When studying the dynamics of a phenomenon, they resort to constructing a time series.
Time series is a series of homogeneous statistical quantities , showing the change of a phenomenon over time and arranged in chronological order at certain intervals. Numbers , components of time series , are called levels.
Row level- size (magnitude) of a phenomenon , achieved during a certain period or at a certain point in time. Series levels can be represented as absolute , relative or average values.
Time series are divided into
A) simple(consisting of absolute values) - can be:
1) momentary- consists of quantities that characterize a phenomenon at a certain moment (statistical information, usually recorded at the beginning or end of a month, quarter, year)
2) interval - consists of numbers characterizing a phenomenon for a certain period of time (interval) - for a week, month, quarter, year (data on the number of births , deaths per year, number of infectious diseases per month). A feature of the interval series is that , that its members can be summed up (in this case the interval becomes larger) or divided.
b) complex(consisting of relative or average values).
Time series can be subject to transformations, the purpose of which is to identify the features of changes in the process being studied, as well as to achieve clarity.
Dynamic series indicators:
A) series levels- values of series members. The value of the first member of the series is called the initial (initial) level, the value of the last member of the series is the final level, the average value of all members of the series is called the average level.
b) absolute increase (decrease)- the magnitude of the difference between the next and previous levels; an increase is expressed in numbers with a positive sign, a decrease - with a negative sign. The value of gain or loss reflects changes in the levels of the dynamic series over a certain period of time.
V) growth rate (decrease)- shows the ratio of each subsequent level to the previous level and is usually expressed as a percentage.
G ) rate of growth (loss)- the ratio of the absolute increase or decrease of each subsequent member of the series to the level of the previous one, expressed as a percentage. The growth rate can also be calculated using the formula: Growth rate - 100%
Absolute value of one percent increase (loss)- is obtained by dividing the absolute value of growth or loss by the rate of growth or loss for the same period.
To more clearly express the increase or decrease of a series, you can transform it by calculating visibility indicators showing the ratio of each member of the series to one of them, taken as one hundred percent.
Sometimes the dynamics of the phenomenon under study are presented not as a continuously changing level, but as separate abrupt changes. In this case, to identify the main trend in the development of the phenomenon being studied, they resort to to align the time series. The following techniques can be used:
A) interval enlargement- summation of data for a number of adjacent periods. The result is totals over longer periods of time. This smooths out random fluctuations and more clearly defines the nature of the dynamics of the phenomenon.
b) calculation of group average- determination of the average value of each enlarged period. To do this, you need to sum up adjacent levels of adjacent periods, and then divide the sum by the number of terms. This provides greater clarity of changes over time.
V) moving average calculation- to some extent eliminates the influence of random fluctuations on the levels of the time series and more noticeably reflects the trend of the phenomenon. When calculating it, each level of the series is replaced by the average value from this level and two adjacent to it. Most often, three terms of the series are summed sequentially, but more can be taken
G) graphic method- alignment by hand or using a ruler or compass of a graphical representation of the dynamics of the phenomenon being studied.
d) least squares alignment- one of the most accurate ways to align a time series. The method aims to eliminate the influence of temporary causes , random factors and identify the main trend in the dynamics of the phenomenon caused by the influence of only long-acting factors. Alignment is carried out along the line that most corresponds to the nature of the dynamics of the phenomenon being studied, if there is a main tendency towards an increase or decrease in the frequency of the phenomenon. This line is usually a straight line , which most accurately characterizes the main direction of change, however, there are other dependencies (quadratic, cubic, etc.). This method allows you to quantify the identified trend, estimate the average rate of its development and calculate projected levels for the next year.
Primary incidence– a set of new, previously unaccounted for diseases identified and registered among the population for the first time in a given calendar year, calculated per 100 thousand population.
General morbidity– the totality of all diseases existing among the population, both first identified in a given calendar year, and registered in previous years, for which patients returned again in a given year.
Cumulative morbidity is the totality of all primary diseases registered over a number of years (minimum 3 years).
Pathological affection– the totality of all pathological conditions (acute and chronic, premorbid conditions) identified during one-time examinations and preventive examinations.
Injuries
Medical and social significance:
1. Injuries and poisonings occupy 2nd place in the structure of morbidity (4 in children), and their growth is observed. 30% of all outpatients and 50% of inpatient surgical patients are treated for injuries.
2. Injuries and poisonings occupy 5th place in the structure of morbidity, their increase is observed (in children - 6).
3. Injuries and poisoning are one of the main causes (3rd place) in the structure of morbidity with temporary disability.
4. Injuries and poisonings occupy 3-4 places in the structure of overall mortality, and their growth is observed. It is the leading cause of death among people of working age.
5. They occupy 3rd-4th place in the structure of disability, and their growth is observed.
6. 70% of all injuries in men and 56% in women occur during working age.
7. Injuries and poisonings are more often recorded in men, especially in working age. At the age of 55 years and more often in women (estrogenic protection decreases).
8. Cause significant economic costs.
Medical and social conditions:
Natural-climatic, biological, and temporary factors play a role in the occurrence of injuries (more on weekends, in the city in winter, in rural areas in summer). Alcohol – 40% is the cause of death from herbs, 24% of transport injuries, 14% of non-occupational injuries.
Most injuries are caused by not so much an increase in trauma-hazards of the environment, but rather a low tolerance of the population to their effects (i.e., low trauma-protection of the population). Low tolerance is due to lifestyle: national diet, alcohol. It also affects subsequent wound healing. Low tolerance is associated with insufficient medical literacy of the population.
50) Malignant neoplasms as a social and hygienic problem.
Malignant neoplasms as a medical and social problem. Main directions of prevention. Organization cancer care.
Malignant neoplasms as a medical and social problem:
1. Cancer is more common in older people.
2. Oncology is a hot spot in medicine.
3. In the structure of overall mortality, oncology makes up 14%.
4. Medical and social significance: patients are incapacitated for a long time, and in a later period they become disabled.
5. Every year, out of 10 thousand workers, 78 go on disability. In overall mortality - 3rd place.
6. Late diagnosis, because Initially, malignant neoplasms are asymptomatic.
7. High costs for diagnosis and treatment of oncology.
Organization of cancer care in the Republic of Belarus: If a local doctor suspects cancer, he or she will refer you for a consultation with a surgeon. The surgeon sends the patient to the oncology clinic (in the Republic of Belarus - 11). There is also an institute of oncology and medical radiology, and a children's oncology and hematology center.
Main directions of prevention- as with BSK.
Health Economics.
Health Economics- a branch of the science of economics that studies the place of health care in national economy, developing methods rational use resources to ensure public health protection.
Purpose of Health Economics- meeting the population's need for medical care.
Subject of Health Economics- development of methods for rational use of resources to achieve goals in protecting public health.
Health economics studies conditions and factors that ensure maximum satisfaction of the population's needs for goods and services necessary to preserve, strengthen, and restore health, at minimal cost. Economists study the impact of population health on the economic development of the country, regions, production, etc., as well as the economic effect of medical and preventive services, prevention, diagnosis, treatment, rehabilitation, elimination of diseases, reduction of disability and mortality, new methods, technologies, organizational events, programs, etc.
Health economics methods:
1) Analysis and synthesis. In the process of analysis, thinking goes from the general to the specific, i.e. the phenomenon under study is divided into its component parts and aspects. Synthesis implies the integration of particular concepts and properties into the general to identify the most significant patterns.
2) Mathematical and statistical techniques and research tools - help to reveal the quantitative relationship of economic variables. Revealing quantitative changes in processes, health care economics also explores the transition of quantity into a new quality. Mathematical and statistical analysis reveals real relationships only when it is closely related to the qualitative content of the subject being analyzed.
3) The balance sheet method is a set of methods of economic calculations. They are used to ensure a strictly defined quantitative relationship between any components, for example, between needs and the possibilities of meeting them, between the revenue and expenditure parts of the budget, etc. The method of economic balances is based on the principle of equality of the values of resources and the possibilities of their use, taking into account the creation of reserves. The latter is very important, because Without reserves, in conditions of a sharp shortage of resources, one or another functional block of the healthcare system may fail, which is fraught with serious medical and social consequences.
4) Forecasting - represents the scientific prediction of the most likely changes in the state of the healthcare industry, society's needs for medical services, production capabilities of medicine, directions of technical progress of the industry, etc.
5) Economic experiments are one of the currently widespread methods. They are reasonable and necessary. The search for certain methods of increasing the efficiency of the healthcare system using the example of several regions or individual medical institutions is of great practical importance.
Insurance form ZO.
Types of insurance: compulsory and voluntary health insurance.
Sources of financing insurance medicine:
1) insurance premiums from enterprises and organizations
2) insurance premiums from citizens
3) state subsidies to insurance companies - for servicing the uninsured
Public health and healthcare as a science and subject of teaching.
Public health and healthcare is the science and specific activities to protect and strengthen the health of the population, prolong life through mobilizing the efforts of society and carrying out relevant organizational activities at various levels.
Public health is an area of scientific and practical activity that ensures the management of health care as one of the largest social systems, where medicine is one of the components along with economics, sociology, political sciences, and industry.
Subject of science.
Science studies patterns of public health and healthcare.
Items:
1. Public health.
2. Healthcare.
3. Factors influencing public health.
4. Medically and socially significant pathology.
1. Public health– a medical, demographic and social category that reflects the physical, psychological, social well-being of people carrying out their life activities within the framework of the definition of social communities.
2. Healthcare is a system of socio-economic and medical measures aimed at preserving and improving the level of health of each person and the population as a whole (BME, 3rd ed.)
3.Risk factors– potentially hazardous factors to health of a behavioral, biological, genetic, environmental, social nature, environmental and industrial environment, increasing the likelihood of developing diseases, their progression and unfavorable outcome.
I. Socio-economic factors.
1. The level of productive forces and the nature of production relations.
2. Organization of medical care.
3. Health care legislation.
4. Lifestyle and conditions.
II. Natural and climatic.
III. Biological: gender, age, constitution, heredity.
IV. Psycho-emotional.
Health formula (in%): 50 – lifestyle, 20 – heredity, 20 – environment, 10 – health activities.
4. Socially significant diseases– diseases caused primarily by socio-economic conditions, causing damage to society and requiring social protection of a person.
Objectives of science:
1. Assessment and study of population health, the dynamics of its development.
2. Assessment and study of social and other conditions affecting health.
3. Development of methods and methods for promoting health, preventing diseases and disabilities, as well as their rehabilitation.
4. Theoretical substantiation of development principles, assessment of the quality and effectiveness of healthcare.
5. Solving problems of management, financing and economics of health care.
6. Legal regulation of healthcare.
7. Formation of social and hygienic mentality and thinking of medical workers.
Sections of science:
1. Sanitary statistics (public health).
2. Examination of disability.
3. Organization of medical care (health care).
4. Management, planning, financing, health care economics.